Type 1 diabetes
Updated: 2024-03-27
Overview
Type 1 diabetes, once known as juvenile diabetes or insulin-dependent diabetes, is a chronic condition. In this condition, the pancreas makes little or no insulin. Insulin is a hormone the body uses to allow sugar (glucose) to enter cells to produce energy.
Different factors, such as genetics and some viruses, may cause type 1 diabetes. Although type 1 diabetes usually appears during childhood or adolescence, it can develop in adults.
Even after a lot of research, type 1 diabetes has no cure. Treatment is directed toward managing the amount of sugar in the blood using insulin, diet and lifestyle to prevent complications.
Symptoms
Type 1 diabetes symptoms can appear suddenly and may include:
- Feeling more thirsty than usual
- Urinating a lot
- Bed-wetting in children who have never wet the bed during the night
- Feeling very hungry
- Losing weight without trying
- Feeling irritable or having other mood changes
- Feeling tired and weak
- Having blurry vision
When to see a doctor
Talk to your health care provider if you notice any of the above symptoms in you or your child.
Causes
The exact cause of type 1 diabetes is unknown. Usually, the body's own immune system — which normally fights harmful bacteria and viruses — destroys the insulin-producing (islet) cells in the pancreas. Other possible causes include:
- Genetics
- Exposure to viruses and other environmental factors
The role of insulin
Once a large number of islet cells are destroyed, the body will produce little or no insulin. Insulin is a hormone that comes from a gland behind and below the stomach (pancreas).
- The pancreas puts insulin into the bloodstream.
- Insulin travels through the body, allowing sugar to enter the cells.
- Insulin lowers the amount of sugar in the bloodstream.
- As the blood sugar level drops, the pancreas puts less insulin into the bloodstream.
The role of glucose
Glucose — a sugar — is a main source of energy for the cells that make up muscles and other tissues.
- Glucose comes from two major sources: food and the liver.
- Sugar is absorbed into the bloodstream, where it enters cells with the help of insulin.
- The liver stores glucose in the form of glycogen.
- When glucose levels are low, such as when you haven't eaten in a while, the liver breaks down the stored glycogen into glucose. This keeps glucose levels within a typical range.
In type 1 diabetes, there's no insulin to let glucose into the cells. Because of this, sugar builds up in the bloodstream. This can cause life-threatening complications.
Risk factors
Some factors that can raise your risk for type 1 diabetes include:
- Family history. Anyone with a parent or sibling with type 1 diabetes has a slightly higher risk of developing the condition.
- Genetics. Having certain genes increases the risk of developing type 1 diabetes.
- Geography. The number of people who have type 1 diabetes tends to be higher as you travel away from the equator.
- Age. Type 1 diabetes can appear at any age, but it appears at two noticeable peaks. The first peak occurs in children between 4 and 7 years old. The second is in children between 10 and 14 years old.
Complications
Over time, type 1 diabetes complications can affect major organs in the body. These organs include the heart, blood vessels, nerves, eyes and kidneys. Having a normal blood sugar level can lower the risk of many complications.
Diabetes complications can lead to disabilities or even threaten your life.
- Heart and blood vessel disease. Diabetes increases the risk of some problems with the heart and blood vessels. These include coronary artery disease with chest pain (angina), heart attack, stroke, narrowing of the arteries (atherosclerosis) and high blood pressure.
-
Nerve damage (neuropathy). Too much sugar in the blood can injure the walls of the tiny blood vessels (capillaries) that feed the nerves. This is especially true in the legs. This can cause tingling, numbness, burning or pain. This usually begins at the tips of the toes or fingers and spreads upward. Poorly controlled blood sugar could cause you to lose all sense of feeling in the affected limbs over time.
Damage to the nerves that affect the digestive system can cause problems with nausea, vomiting, diarrhea or constipation. For men, erectile dysfunction may be an issue.
- Kidney damage (nephropathy). The kidneys have millions of tiny blood vessels that keep waste from entering the blood. Diabetes can damage this system. Severe damage can lead to kidney failure or end-stage kidney disease that can't be reversed. End-stage kidney disease needs to be treated with mechanical filtering of the kidneys (dialysis) or a kidney transplant.
- Eye damage. Diabetes can damage the blood vessels in the retina (part of the eye that senses light) (diabetic retinopathy). This could cause blindness. Diabetes also increases the risk of other serious vision conditions, such as cataracts and glaucoma.
- Foot damage. Nerve damage in the feet or poor blood flow to the feet increases the risk of some foot complications. Left untreated, cuts and blisters can become serious infections. These infections may need to be treated with toe, foot or leg removal (amputation).
- Skin and mouth conditions. Diabetes may leave you more prone to infections of the skin and mouth. These include bacterial and fungal infections. Gum disease and dry mouth also are more likely.
- Pregnancy complications. High blood sugar levels can be dangerous for both the parent and the baby. The risk of miscarriage, stillbirth and birth defects increases when diabetes isn't well-controlled. For the parent, diabetes increases the risk of diabetic ketoacidosis, diabetic eye problems (retinopathy), pregnancy-induced high blood pressure and preeclampsia.
Prevention
There's no known way to prevent type 1 diabetes. But researchers are working on preventing the disease or further damage of the islet cells in people who are newly diagnosed.
Ask your provider if you might be eligible for one of these clinical trials. It is important to carefully weigh the risks and benefits of any treatment available in a trial.
Diagnosis
Diagnostic tests include:
- Glycated hemoglobin (A1C) test. This blood test shows your average blood sugar level for the past 2 to 3 months. It measures the amount of blood sugar attached to the oxygen-carrying protein in red blood cells (hemoglobin). The higher the blood sugar levels, the more hemoglobin you'll have with sugar attached. An A1C level of 6.5% or higher on two separate tests means you have diabetes.
If the A1C test isn't available, or if you have certain conditions that can make the A1C test inaccurate — such as pregnancy or an uncommon form of hemoglobin (hemoglobin variant) — your provider may use these tests:
- Random blood sugar test. A blood sample will be taken at a random time and may be confirmed by additional tests. Blood sugar values are expressed in milligrams per deciliter (mg/dL) or millimoles per liter (mmol/L). No matter when you last ate, a random blood sugar level of 200 mg/dL (11.1 mmol/L) or higher suggests diabetes.
- Fasting blood sugar test. A blood sample will be taken after you don't eat (fast) overnight. A fasting blood sugar level less than 100 mg/dL (5.6 mmol/L) is healthy. A fasting blood sugar level from 100 to 125 mg/dL (5.6 to 6.9 mmol/L) is considered prediabetes. If it's 126 mg/dL (7 mmol/L) or higher on two separate tests, you have diabetes.
If you're diagnosed with diabetes, your provider may also run blood tests. These will check for autoantibodies that are common in type 1 diabetes. The tests help your provider decide between type 1 and type 2 diabetes when the diagnosis isn't certain. The presence of ketones — byproducts from the breakdown of fat — in your urine also suggests type 1 diabetes, rather than type 2.
After the diagnosis
You'll regularly visit your provider to talk about managing your diabetes. During these visits, the provider will check your A1C levels. Your target A1C goal may vary depending on your age and various other factors. The American Diabetes Association generally recommends that A1C levels be below 7%, or an average glucose level of about 154 mg/dL (8.5 mmol/L).
A1C testing shows how well the diabetes treatment plan is working better than daily blood sugar tests. A high A1C level may mean you need to change the insulin amount, meal plan or both.
Your provider will also take blood and urine samples. They will use these samples to check cholesterol levels, as well as thyroid, liver and kidney function. Your provider will also take your blood pressure and check the sites where you test your blood sugar and deliver insulin.
Treatment
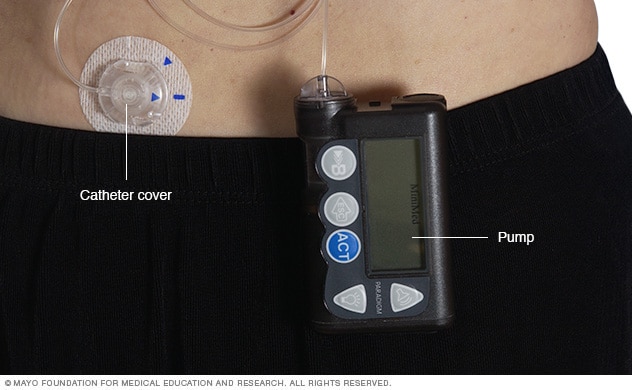
Insulin pump
An insulin pump is a device about the size of a cellphone that's worn on the outside of your body. A tube connects the reservoir of insulin to a catheter that's inserted under the skin of your abdomen. Insulin pumps are programmed to dispense specific amounts of insulin automatically and when you eat.
Treatment for type 1 diabetes includes:
- Taking insulin
- Counting carbohydrates, fats and protein
- Monitoring blood sugar often
- Eating healthy foods
- Exercising regularly and keeping a healthy weight
The goal is to keep the blood sugar level as close to normal as possible to delay or prevent complications. Generally, the goal is to keep the daytime blood sugar levels before meals between 80 and 130 mg/dL (4.44 to 7.2 mmol/L). After-meal numbers should be no higher than 180 mg/dL (10 mmol/L) two hours after eating.
Insulin and other medications
Anyone who has type 1 diabetes needs insulin therapy throughout their life.
There are many types of insulin, including:
- Short-acting insulin. Sometimes called regular insulin, this type starts working around 30 minutes after injection. It reaches peak effect at 90 to 120 minutes and lasts about 4 to 6 hours. Examples are Humulin R, Novolin R and Afrezza.
- Rapid-acting insulin. This type of insulin starts working within 15 minutes. It reaches peak effect at 60 minutes and lasts about 4 hours. This type is often used 15 to 20 minutes before meals. Examples are glulisine (Apidra), lispro (Humalog, Admelog and Lyumjev) and aspart (Novolog and FiAsp).
- Intermediate-acting insulin. Also called NPH insulin, this type of insulin starts working in about 1 to 3 hours. It reaches peak effect at 6 to 8 hours and lasts 12 to 24 hours. Examples are insulin NPH (Novolin N, Humulin N).
- Long- and ultra-long-acting insulin. This type of insulin may provide coverage for as long as 14 to 40 hours. Examples are glargine (Lantus, Toujeo Solostar, Basaglar), detemir (Levemir) and degludec (Tresiba).
You'll probably need several daily injections that include a combination of a long-acting insulin and a rapid-acting insulin. These injections act more like the body's normal use of insulin than do older insulin regimens that only required one or two shots a day. A combination of three or more insulin injections a day has been shown to improve blood sugar levels.
Insulin delivery options
Insulin can't be taken by mouth to lower blood sugar because stomach enzymes will break down the insulin, preventing it from working. You'll need to either get shots (injections) or use an insulin pump.
-
Injections. You can use a fine needle and syringe or an insulin pen to inject insulin under the skin. Insulin pens look like ink pens and are available in disposable or refillable varieties.
If you choose shots (injections), you'll probably need a mixture of insulin types to use during the day and night.
-
An insulin pump. This is a small device worn on the outside of your body that you program to deliver specific amounts of insulin throughout the day and when you eat. A tube connects a reservoir of insulin to a catheter that's inserted under the skin of your abdomen.
There's also a tubeless pump option that involves wearing a pod containing the insulin on your body combined with a tiny catheter that's inserted under your skin.
Blood sugar monitoring
Depending on the type of insulin therapy you select or need, you may have to check and record your blood sugar level at least four times a day.
The American Diabetes Association recommends testing blood sugar levels before meals and snacks, before bed, before exercising or driving, and whenever you think you have low blood sugar. Careful monitoring is the only way to make sure that your blood sugar level remains within your target range. More frequent monitoring can lower A1C levels.
Even if you take insulin and eat on a strict schedule, blood sugar levels can change. You'll learn how your blood sugar level changes in response to food, activity, illness, medications, stress, hormonal changes and alcohol.
Continuous glucose monitoring
Continuous glucose monitoring (CGM) monitors blood sugar levels. It may be especially helpful for preventing low blood sugar. These devices have been shown to lower A1C.
Continuous glucose monitors attach to the body using a fine needle just under the skin. They check blood glucose levels every few minutes.
Closed loop system
A closed loop system is a device implanted in the body that links a continuous glucose monitor to an insulin pump. The monitor checks blood sugar levels regularly. The device automatically delivers the right amount of insulin when the monitor shows that it's needed.
The Food and Drug Administration has approved several hybrid closed loop systems for type 1 diabetes. They are called "hybrid" because these systems require some input from the user. For example, you may have to tell the device how many carbohydrates are eaten, or confirm blood sugar levels from time to time.
A closed loop system that doesn't need any user input isn't available yet. But more of these systems currently are in clinical trials.
Other medications
Other medications also may be prescribed for people with type 1 diabetes, such as:
- High blood pressure medications. Your provider may prescribe angiotensin-converting enzyme (ACE) inhibitors or angiotensin II receptor blockers (ARBs) to help keep your kidneys healthy. These medications are recommended for people with diabetes who have blood pressures above 140/90 millimeters of mercury (mm Hg).
- Aspirin. Your provider may recommend you take baby or regular aspirin daily to protect your heart. Your provider may feel that you have an increased risk of a cardiovascular event. Your provider will discuss the risk of bleeding if you take aspirin.
-
Cholesterol-lowering drugs. Cholesterol guidelines are stricter for people with diabetes because of their higher risk of heart disease.
The American Diabetes Association recommends that low-density lipoprotein (LDL, or "bad") cholesterol be below 100 mg/dL (2.6 mmol/L). High-density lipoprotein (HDL, or "good") cholesterol is recommended to be over 50 mg/dL (1.3 mmol/L) in women and over 40 mg/dL (1 mmol/L) in men. Triglycerides, another type of blood fat, should be less than 150 mg/dL (1.7 mmol/L).
Healthy eating and monitoring carbohydrates
There's no such thing as a diabetes diet. However, it's important to center your diet on nutritious, low-fat, high-fiber foods such as:
- Fruits
- Vegetables
- Whole grains
Your registered dietitian will recommend that you eat fewer animal products and refined carbohydrates, such as white bread and sweets. This healthy-eating plan is recommended even for people without diabetes.
You'll need to learn how to count the amount of carbohydrates in the foods you eat. By doing so, you can give yourself enough insulin. This will allow your body to properly use those carbohydrates. A registered dietitian can help you create a meal plan that fits your needs.
Physical activity
Everyone needs regular aerobic exercise, including people who have type 1 diabetes. First, get your provider's OK to exercise. Then choose activities you enjoy, such as walking or swimming, and do them every day when you can. Try for at least 150 minutes of moderate aerobic exercise a week, with no more than two days without any exercise.
Remember that physical activity lowers blood sugar. If you begin a new activity, check your blood sugar level more often than usual until you know how that activity affects your blood sugar levels. You might need to adjust your meal plan or insulin doses because of the increased activity.
Activities of concern
Certain life activities may be of concern for people who have type 1 diabetes.
- Driving. Low blood sugar can occur at any time. It's a good idea to check your blood sugar anytime you're getting behind the wheel. If it's below 70 mg/dL (3.9 mmol/L), have a snack with 15 grams of carbohydrates. Retest again in 15 minutes to make sure it has risen to a safe level before you start driving.
- Working. Type 1 diabetes can pose some challenges in the workplace. For example, if you work in a job that involves driving or operating heavy machinery, low blood sugar could pose a serious risk to you and those around you. You may need to work with your provider and your employer to ensure that certain adjustments are made. You may need additional breaks for blood sugar testing and fast access to food and drink. There are federal and state laws that require employers to provide these adjustments for people with diabetes.
-
Being pregnant. The risk of complications during pregnancy is higher for people with type 1 diabetes. Experts recommend that you see your provider before you get pregnant. A1C readings should be less than 6.5% before you try to get pregnant.
The risk of diseases present at birth (congenital diseases) is higher for people with type 1 diabetes. The risk is higher when diabetes is poorly controlled during the first 6 to 8 weeks of pregnancy. Careful management of your diabetes during pregnancy can lower your risk of complications.
- Being older or having other conditions. For those who are weak or sick or have difficulty thinking clearly, tight control of blood sugar may not be practical. It could also increase the risk of low blood sugar. For many people with type 1 diabetes, a less strict A1C goal of less than 8% may be appropriate.
Potential future treatments
- Pancreas transplant. With a successful pancreas transplant, you would no longer need insulin. But pancreas transplants aren't always successful — and the procedure poses serious risks. Because these risks can be more dangerous than the diabetes itself, pancreas transplants are generally used for those with very difficult-to-manage diabetes. They can also be used for people who also need a kidney transplant.
- Islet cell transplantation. Researchers are experimenting with islet cell transplantation. This provides new insulin-producing cells from a donor pancreas. This experimental procedure had some problems in the past. But new techniques and better drugs to prevent islet cell rejection may improve its chances of becoming a successful treatment.
Signs of trouble
Despite your best efforts, sometimes problems will happen. Certain short-term complications of type 1 diabetes, such as low blood sugar, require care immediately.
Low blood sugar (hypoglycemia)
Diabetic hypoglycemia occurs when someone with diabetes doesn't have enough sugar (glucose) in the blood. Ask your provider what's considered a low blood sugar level for you. Blood sugar levels can drop for many reasons, such as skipping a meal, eating fewer carbohydrates than called for in your meal plan, getting more physical activity than normal or injecting too much insulin.
Learn the symptoms of hypoglycemia. Test your blood sugar if you think your levels are low. When in doubt, always test your blood sugar. Early symptoms of low blood sugar include:
- Looking pale (pallor)
- Shakiness
- Dizziness or lightheadedness
- Sweating
- Hunger or nausea
- An irregular or fast heartbeat
- Difficulty concentrating
- Feeling weak and having no energy (fatigue)
- Irritability or anxiety
- Headache
- Tingling or numbness of the lips, tongue or cheek
Nighttime hypoglycemia may cause you to wake with sweat-soaked pajamas or a headache. Nighttime hypoglycemia sometimes might cause an unusually high blood sugar reading first thing in the morning.
If diabetic hypoglycemia isn't treated, symptoms of hypoglycemia worsen and can include:
- Confusion, unusual behavior or both, such as the inability to complete routine tasks
- Loss of coordination
- Difficulty speaking or slurred speech
- Blurry or tunnel vision
- Inability to eat or drink
- Muscle weakness
- Drowsiness
Severe hypoglycemia may cause:
- Convulsions or seizures
- Unconsciousness
- Death, rarely
You can raise your blood sugar quickly by eating or drinking a simple sugar source, such as glucose tablets, hard candy or fruit juice. Tell family and friends what symptoms to look for and what to do if you're not able to treat the condition yourself.
If a blood glucose meter isn't readily available, treat for low blood sugar anyway if you have symptoms of hypoglycemia, and then test as soon as possible.
Inform people you trust about hypoglycemia. If others know what symptoms to look for, they might be able to alert you to early symptoms. It's important that family members and close friends know where you keep glucagon and how to give it so that a potentially serious situation can be easier to safely manage. Glucagon is a hormone that stimulates the release of sugar into the blood.
Here's some emergency information to give to others. If you're with someone who is not responding (loses consciousness) or can't swallow due to low blood sugar:
- Don't inject insulin, as this will cause blood sugar levels to drop even further
- Don't give fluids or food, because these could cause choking
- Give glucagon by injection or a nasal spray
- Call 911 or emergency services in your area for immediate treatment if glucagon isn't on hand, you don't know how to use it or the person isn't responding
Hypoglycemia unawareness
Some people may lose the ability to sense that their blood sugar levels are getting low. This is called hypoglycemia unawareness. The body no longer reacts to a low blood sugar level with symptoms such as lightheadedness or headaches. The more you experience low blood sugar, the more likely you are to develop hypoglycemia unawareness.
If you can avoid having a hypoglycemic episode for several weeks, you may start to become more aware of coming lows. Sometimes increasing the blood sugar target (for example, from 80 to 120 mg/DL to 100 to 140 mg/DL) at least for a short time can also help improve low blood sugar awareness.
High blood sugar (hyperglycemia)
Blood sugar can rise for many reasons. For example, it can rise due to eating too much, eating the wrong types of foods, not taking enough insulin or fighting an illness.
Watch for:
- Frequent urination
- Increased thirst
- Blurred vision
- Fatigue
- Headache
- Irritability
If you think you have hyperglycemia, check your blood sugar. If it is higher than your target range, you'll likely need to administer a "correction." A correction is an additional dose of insulin given to bring your blood sugar back to normal. High blood sugar levels don't come down as quickly as they go up. Ask your provider how long to wait until you recheck. If you use an insulin pump, random high blood sugar readings may mean you need to change the place where you put the pump on your body.
If you have a blood sugar reading above 240 mg/dL (13.3 mmol/L), test for ketones using a urine test stick. Don't exercise if your blood sugar level is above 240 mg/dL or if ketones are present. If only a trace or small amounts of ketones are present, drink extra noncalorie fluids to flush out the ketones.
If your blood sugar is persistently above 300 mg/dL (16.7 mmol/L), or if your urine ketones stays high in spite of taking correction doses of insulin, call your provider or seek emergency care.
Increased ketones in your urine (diabetic ketoacidosis)
If your cells are starved for energy, the body may begin to break down fat. This produces toxic acids known as ketones. Diabetic ketoacidosis is a life-threatening emergency.
Symptoms of this serious condition include:
- Nausea
- Vomiting
- Abdominal pain
- A sweet, fruity smell on your breath
- Shortness of breath
- Dry mouth
- Weakness
- Confusion
- Coma
If you suspect ketoacidosis, check the urine for excess ketones with an over-the-counter ketones test kit. If you have large amounts of ketones in the urine, call your provider right away or seek emergency care. Also, call your provider if you have vomited more than once and you have ketones in the urine.
Lifestyle and home remedies
Careful management of type 1 diabetes can lower your risk of serious — even life-threatening — complications. Consider these tips:
- Make a commitment to manage your diabetes. Take your medications as recommended. Learn all you can about type 1 diabetes. Make healthy eating and physical activity part of your daily routine. Establish a relationship with a diabetes educator. Ask your health care team for help.
- Identify yourself. Wear a tag or bracelet that says you are living with diabetes. Keep a glucagon kit nearby in case of a low blood sugar emergency. Make sure your friends and loved ones know how to use the kit.
- Schedule a yearly physical exam and regular eye exams. Your regular diabetes checkups aren't meant to replace yearly physicals or routine eye exams. During the physical, your provider will look for any diabetes-related complications. Your provider will also look for other medical problems. Your eye care specialist will check for signs of eye complications, such as retina damage, cataracts and glaucoma.
-
Keep your vaccinations up to date. High blood sugar can weaken the immune system. Get a flu shot every year. Your provider will likely recommend the pneumonia vaccine, too. They may also recommend getting the COVID-19 vaccine.
The Centers for Disease Control and Prevention (CDC) recommends hepatitis B vaccination if you haven't had it before and you're an adult between the ages of 19 and 59 years with type 1 or type 2 diabetes. The CDC recommends vaccination as soon as possible after diagnosis with type 1 or type 2 diabetes. If you are age 60 or older and have diabetes and haven't received the vaccine, talk to your provider about whether it's right for you.
- Pay attention to your feet. Wash your feet daily in lukewarm water. Dry them gently, especially between the toes. Moisturize your feet with lotion. Check your feet every day for blisters, cuts, sores, redness or swelling. Consult your provider if you have a sore or other foot problem that doesn't heal.
- Keep your blood pressure and cholesterol under control. Eating healthy foods and exercising regularly can help control high blood pressure and cholesterol. Medication also may be needed.
- If you smoke or use other forms of tobacco, ask your provider to help you quit. Smoking increases your risk of diabetes complications. These include heart attack, stroke, nerve damage and kidney disease. Talk to your provider about ways to stop smoking or to stop using other types of tobacco.
- If you drink alcohol, do so responsibly. Alcohol can cause either high or low blood sugar. It depends on how much you drink and if you eat at the same time. If you choose to drink, do so only in moderation and always with a meal. Check your blood sugar levels before going to sleep.
- Take stress seriously. The hormones the body produces when you're under long-term stress may prevent insulin from working properly. This can stress and frustrate you even more. Take a step back and set some limits. Prioritize your tasks. Learn ways to relax. Get plenty of sleep.
Coping and support
Diabetes can affect emotions both directly and indirectly. Poorly controlled blood sugar can directly affect emotions by causing behavior changes, such as irritability. There may be times when you resent your diabetes.
People living with diabetes have an increased risk of depression and diabetes-related distress. Many diabetes specialists regularly include a social worker or psychologist as part of their diabetes care team.
You may find that it helps to talk to other people with type 1 diabetes. Online and in-person support groups are available. Group members often know about the latest treatments. They may also share their own experiences or helpful information. For example, they may share where to find carbohydrate counts for your favorite takeout restaurant.
If you're interested in a support group, your provider may be able to recommend one in your area. Or you can visit the websites of the American Diabetes Association (ADA) or the Juvenile Diabetes Research Foundation (JDRF). These sites may list support group information and local activities for people with type 1 diabetes. You can also reach the ADA at 800-DIABETES (800-342-2383) or JDRF at 800-533-CURE (800-533-2873).
Preparing for an appointment
If you think that you or your child might have type 1 diabetes, see your provider immediately. A simple blood test can show if you need more evaluation and treatment.
After diagnosis, you'll need close medical follow-up until your blood sugar level is stable. A provider who specializes in hormonal disorders (endocrinologist) usually works with other specialists on diabetes care. Your health care team will likely include:
- Certified diabetes educator
- Registered dietitian
- Social worker or mental health professional
- Pharmacist
- Dentist
- Certified diabetes educator
- Health care provider who specializes in eye care (ophthalmologist)
- Health care provider who specializes in foot health (podiatrist)
Once you've learned how to manage type 1 diabetes, your provider likely will recommend checkups every few months. A thorough yearly exam and regular foot and eye exams also are important. This is especially true if you're having a hard time managing your diabetes, if you have high blood pressure or kidney disease, or if you're pregnant.
These tips can help you prepare for your appointments. They can also let you know what to expect from your provider.
What you can do
- Write down any questions you have. Once you begin insulin treatment, the first symptoms of diabetes should go away. However, you may have new issues that you need to address. These include having low blood sugar that happens often or finding ways to control high blood sugar after eating certain foods.
- Write down key personal information, including any major sources of stress or recent changes in your life. Many factors can affect your diabetes control, including stress.
- Make a list of all the medications, vitamins and supplements you're taking.
- For your regular checkups, bring the records of your glucose values or your meter to your appointments.
- Write down questions to ask your provider.
Preparing a list of questions can help you make the most of your time with your provider and the rest of your health care team. Things you want to discuss with your provider, registered dietitian or diabetes educator include:
- When and how often you should monitor your blood glucose
- Insulin therapy — types of insulin used, timing of dosing, amount of dose
- Insulin administration — shots versus a pump
- Low blood sugar — how to recognize and treat
- High blood sugar — how to recognize and treat
- Ketones — testing and treatment
- Nutrition — types of food and their effect on blood sugar
- Carbohydrate counting
- Exercise — adjusting insulin and food intake for activity
- Medical management — how often to visit your provider and other diabetes care team members
- Sick day management
What to expect from your doctor
Your provider is likely to ask you many questions, including:
- How comfortable are you managing your diabetes?
- How frequent are your low blood sugar episodes?
- Do you know when your blood sugar is getting low?
- What's a typical day's diet like?
- Are you exercising? If so, how often?
- On average, how much insulin are you using daily?
What you can do in the meantime
If you're having trouble managing your blood sugar or you have questions, contact your health care team in between appointments.