Obstructive sleep apnea
Updated: 2023-07-14
Overview
Obstructive sleep apnea
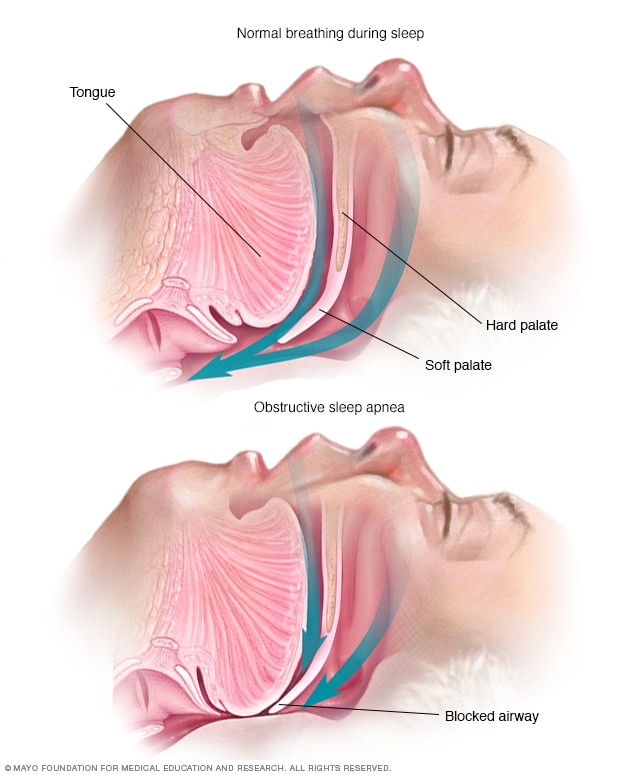
Obstructive sleep apnea occurs when the muscles that support the soft tissues in your throat, such as your tongue and soft palate, temporarily relax. When these muscles relax, your airway is narrowed or closed, and breathing is momentarily cut off.
Obstructive sleep apnea is the most common sleep-related breathing disorder. People with obstructive sleep apnea repeatedly stop and start breathing while they sleep.
There are several types of sleep apnea. Obstructive sleep apnea occurs when the throat muscles relax and block the airway. This happens off and on many times during sleep. A sign of obstructive sleep apnea is snoring.
Treatments for obstructive sleep apnea are available. One treatment is a device that uses positive pressure to keep the airway open during sleep. Another option is a mouthpiece to thrust the lower jaw forward during sleep. In some people, surgery might be an option too.
Symptoms
Symptoms of obstructive sleep apnea include:
- Excessive daytime sleepiness.
- Loud snoring.
- Observed episodes of stopped breathing during sleep.
- Waking during the night and gasping or choking.
- Awakening in the morning with a dry mouth or sore throat.
- Morning headaches.
- Trouble focusing during the day.
- Mood changes, such as depression or being easily upset.
- High blood pressure.
- Decreased interest in sex.
When to see a doctor
Consult a health care professional if you have, or if your partner observes, the following:
- Snoring loud enough to disturb your sleep or the sleep of others.
- Waking up gasping or choking.
- Pausing in your breathing during sleep.
- Having excessive daytime drowsiness. This may cause you to fall asleep while working, watching television or even driving a vehicle.
Snoring doesn't necessarily indicate something potentially serious, and not everyone who snores has obstructive sleep apnea.
Be sure to talk to a member of your health care team if you snore loudly, especially if your snoring is interrupted by periods of silence. Snoring may be loudest — and breath pauses known as apneas may be more common — when you sleep on your back.
Ask your health care team about any sleep problem that leaves you fatigued, sleepy and irritable on a regular basis. Excessive daytime drowsiness may be due to other disorders, such as narcolepsy.
Causes
Obstructive sleep apnea occurs when the muscles in the back of the throat relax too much to allow for proper breathing. These muscles support the back of the roof of the mouth, known as the soft palate. The muscles also support the tongue and side walls of the throat.
When the muscles relax, the airway narrows or closes as you breathe in. This can lower the level of oxygen in the blood and cause a buildup of carbon dioxide.
Your brain senses this impaired breathing and briefly rouses you from sleep so that you can reopen your airway. This awakening is usually so brief that you don't remember it.
You may awaken with shortness of breath that corrects itself quickly, within one or two deep breaths. Or you might make a snorting, choking or gasping sound.
This pattern can repeat itself 5 to 30 times or more each hour, all night long. These disruptions impair your ability to reach the deep, restful phases of sleep, and you'll probably feel sleepy during your waking hours.
People with obstructive sleep apnea might not be aware of their interrupted sleep. Many people with this type of sleep apnea don't realize they haven't slept well all night.
Risk factors
Anyone can develop obstructive sleep apnea. However, certain factors put you at increased risk, including:
- Excess weight. Most but not all people with obstructive sleep apnea are overweight. Fat deposits around the upper airway can obstruct breathing. Medical conditions that are associated with obesity, such as hypothyroidism and polycystic ovary syndrome, also can cause obstructive sleep apnea.
- Older age. The risk of obstructive sleep apnea increases as you age but appears to level off after your 60s and 70s.
- Narrowed airway. A naturally narrow airway is a trait that can be passed down in your family. Or your tonsils or adenoids might become enlarged and block your airway.
- High blood pressure, known as hypertension. Obstructive sleep apnea is relatively common in people with hypertension.
- Chronic nasal congestion. Obstructive sleep apnea occurs twice as often in those who have consistent nasal congestion at night, regardless of the cause.
- Smoking. People who smoke are more likely to have obstructive sleep apnea.
- Diabetes. Obstructive sleep apnea might be more common in people with diabetes.
- Male sex. In general, men are 2 to 3 times more likely as premenopausal women to have obstructive sleep apnea. However, the risk of obstructive sleep apnea increases in women after menopause.
- A family history of sleep apnea. Having family members with obstructive sleep apnea might increase your risk.
- Asthma. Research has found an association between asthma and the risk of obstructive sleep apnea.
Complications
Obstructive sleep apnea is considered a serious medical condition. Complications can include:
-
Daytime fatigue and sleepiness. Because of a lack of restorative sleep at night, people with obstructive sleep apnea often have severe daytime drowsiness, fatigue and irritability. They might have difficulty concentrating and find themselves falling asleep at work, while watching TV or even when driving. This can put them at higher risk of work-related accidents.
Children and young people with obstructive sleep apnea might do poorly in school and commonly have attention or behavior problems.
-
Cardiovascular problems. Sudden drops in blood oxygen levels that occur during obstructive sleep apnea increase blood pressure and strain the cardiovascular system. Many people with obstructive sleep apnea develop high blood pressure, which can increase the risk of heart disease.
The worse the obstructive sleep apnea, the greater the risk of coronary artery disease, heart attack, heart failure and stroke.
Obstructive sleep apnea also increases the risk of heart rhythm problems known as arrhythmias. Arrhythmias can lower blood pressure. If there's underlying heart disease, these repeated multiple episodes of arrhythmias could lead to sudden death.
-
Complications with medicines and surgery. Obstructive sleep apnea also is a concern with certain medicines and general anesthesia. Medicines such as sedatives, some prescription painkillers and general anesthetics, relax the upper airway and can make obstructive sleep apnea worse.
If you have obstructive sleep apnea, having major surgery can worsen breathing problems. This is especially true if you have been sedated and you were lying on your back. People with obstructive sleep apnea might be more prone to complications after surgery.
Before you have surgery, tell your surgeon if you have obstructive sleep apnea or symptoms related to the condition. You may need to get tested for obstructive sleep apnea before surgery.
- Eye problems. Some research has found a connection between obstructive sleep apnea and certain eye conditions, such as glaucoma. Eye complications can usually be treated.
- Sleep-deprived partners. Loud snoring can keep those around you from getting good rest and eventually disrupt your relationships. Some partners choose to sleep in another room.
People with obstructive sleep apnea also may complain of memory problems, morning headaches, and mood swings or depression. They also may need to urinate often at night.
Obstructive sleep apnea might be a risk factor for COVID-19. People with obstructive sleep apnea have been found to be at higher risk for developing a severe form of COVID-19. They may be more likely to need hospital treatment than do those who don't have obstructive sleep apnea.
Diagnosis
A member of your health care team evaluates your condition based on your symptoms, an exam, and tests. You may be referred to a sleep specialist for further evaluation.
The physical exam involves an examination of the back of your throat, mouth and nose. Your neck and waist circumference may be measured. Your blood pressure also may be checked.
A sleep specialist can further evaluate you. The specialist can diagnose and determine the extent of your condition. The specialist also can plan your treatment. The evaluation might involve staying at a sleep center overnight. At the sleep center, your breathing and other body functions are monitored as you sleep.
Tests
Tests to detect obstructive sleep apnea include:
-
Polysomnography. During this sleep study, you're hooked up to equipment that monitors your heart, lung and brain activity and breathing patterns while you sleep. The equipment also measures arm and leg movements and blood oxygen levels.
You might be monitored all night or part of the night. If you're monitored for part of the night, it's called a split-night sleep study.
In a split-night sleep study, you'll be monitored during the first half of the night. If you're diagnosed with obstructive sleep apnea, staff members may wake you and give you continuous positive airway pressure for the second half of the night
The sleep study also can help look for other sleep disorders that can cause excessive daytime sleepiness but have different treatments. The sleep study can uncover leg movements during sleep, known as periodic limb movement disorder. Or the study can help evaluate people who have sudden bouts of sleep during the day, known as narcolepsy.
- Home sleep apnea testing. Under certain circumstances, you may have an at-home version of polysomnography to diagnose obstructive sleep apnea. Home sleep apnea testing kits monitor a limited number of variables to detect breathing pauses during sleep.
Treatment

Continuous positive airway pressure (CPAP)
To eliminate snoring and prevent sleep apnea, a health care professional may recommend a device called a continuous positive airway pressure (CPAP) machine. A CPAP machine delivers just enough air pressure to a mask to keep the upper airway passages open, preventing snoring and sleep apnea.
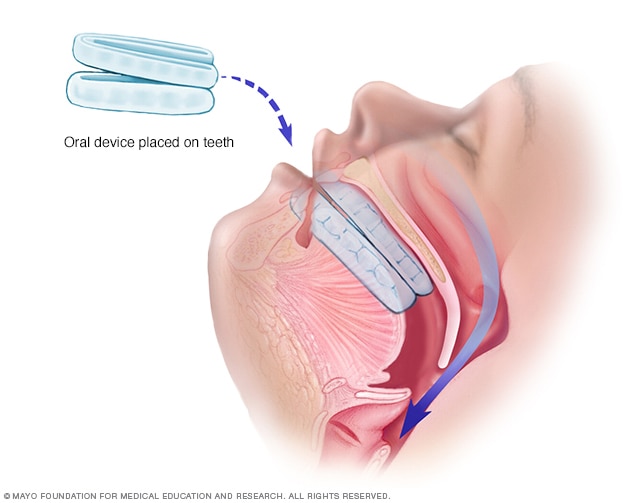
Oral device
An oral device is placed on the teeth and is designed to keep the throat open by moving the tongue and lower jaw forward.

Airway stimulation system
An impulse generator is implanted in the chest and stimulates the nerve that controls tongue movements.

Upper jaw advancement
Upper jaw advancement surgery involves moving the jaw to reduce the risk of obstruction.
Therapies
-
Positive airway pressure. If you have obstructive sleep apnea, you may benefit from positive airway pressure. In this treatment, a machine delivers air pressure through a piece that fits into your nose or is placed over your nose and mouth while you sleep.
Positive airway pressure reduces the number of times you stop breathing as you sleep. The therapy also reduces daytime sleepiness and improves your quality of life.
The most common type is called continuous positive airway pressure, also known as CPAP (SEE-pap). With this treatment, the pressure of the air breathed is continuous, constant and somewhat greater than that of the surrounding air. The pressure of the air is just enough to keep your upper airway passages open. This air pressure prevents obstructive sleep apnea and snoring.
Although CPAP is the most successful and commonly used method of treating obstructive sleep apnea, some people find the mask uncomfortable or loud. However, newer machines are smaller and less noisy than older machines. And there are a variety of mask designs for individual comfort.
Also, with some practice, most people learn to adjust the mask to obtain a comfortable and secure fit. You may need to try different types to find a suitable mask. Several options are available, such as nasal masks, nasal pillows or face masks.
If you're having trouble tolerating pressure, some machines have special adaptive pressure functions to improve comfort. You might also benefit from using a humidifier along with your CPAP system.
CPAP may be given at a continuous pressure, known as fixed. Or the pressure may be varied, known as autotitrating positive airway pressure (APAP). In fixed CPAP, the pressure stays constant. In autotitrating CPAP, the levels of pressure are adjusted if the device senses increased airway resistance.
Bilevel positive airway pressure (BPAP) is another type of positive airway pressure. BPAP delivers a preset amount of pressure when you breathe in and a different amount of pressure when you breathe out.
CPAP is more commonly used because it's been well studied for obstructive sleep apnea and has been shown to effectively treat the condition. People who have difficulty tolerating fixed CPAP might want to try BPAP or APAP.
Don't stop using your positive airway pressure machine if you have problems. Check with your health care team to see what adjustments you can make to improve its comfort.
In addition, contact your health care team if you still snore despite treatment, if you begin snoring again, or if your weight goes up or down by 10% or more.
-
Mouthpiece, known as an oral device. Though positive airway pressure is often an effective treatment, oral appliances are an alternative for some people with mild or moderate obstructive sleep apnea. They're also used for people with severe sleep apnea who can't use CPAP. The devices may reduce sleepiness and improve quality of life.
These devices are designed to keep the throat open. Some devices keep the airway open by bringing the lower jaw forward, which can sometimes relieve snoring and obstructive sleep apnea. Other devices hold the tongue in a different position.
If you decide to explore this option, you'll need to see a dentist experienced in dental sleep medicine appliances for the fitting and follow-up therapy. A number of devices are available. Close follow-up is needed to ensure successful treatment and that use of the device doesn't cause changes to your teeth.
A newer device uses electrical stimulation on the tongue. The device helps improve snoring and breathing during sleep in people with very mild sleep apnea and snoring. This device isn't meant to be used in place of CPAP when it's recommended for moderate to severe obstructive sleep apnea.
It's a removable device that you place around your tongue while you're awake. It delivers electrical impulses to improve the muscle tone of the tongue. This helps prevent the tongue from collapsing and blocking the airway during sleep. The device is used for 20 minutes a day. It takes six weeks to see improvement. A dentist makes a custom device that fits you.
Only a small number of studies has looked at how well these devices work. Larger studies are still needed. Don't use a tongue muscle stimulation device if you have a pacemaker or another implanted electrical device.
Surgery or other procedures
Surgery is usually considered only if other therapies haven't been effective or haven't been appropriate options for you. Surgical options may include:
- Surgical removal of tissue. Uvulopalatopharyngoplasty (UPPP) is a procedure in which a surgeon removes tissue from the back of the mouth and top of the throat. The tonsils and adenoids may be removed as well. UPPP usually is performed in a hospital and requires a medicine that puts you in a sleep-like state. This medicine is called a general anesthetic.
-
Upper airway stimulation. This new device is approved for use in people with moderate to severe obstructive sleep apnea who can't tolerate CPAP or BPAP.
A small, thin impulse generator, known as a hypoglossal nerve stimulator, is implanted under the skin in the upper chest. When you inhale, the device stimulates the nerve that controls the movement of the tongue. The tongue moves forward instead of moving backward and blocking the throat.
Studies have found that upper airway stimulation greatly improves obstructive sleep apnea symptoms and quality of life.
- Jaw surgery, known as maxillomandibular advancement. In this procedure, the upper and lower parts of the jaw are moved forward compared with the rest of the facial bones. This enlarges the space behind the tongue and soft palate, making obstruction less likely.
-
Surgical opening in the neck, known as a tracheostomy. You may need this form of surgery if other treatments have failed and you have life-threatening obstructive sleep apnea.
During a tracheostomy, a surgeon makes an opening in the neck and inserts a metal or plastic tube for breathing. Air passes in and out of the lungs, bypassing the blocked air passage in your throat.
Other types of surgery may help reduce snoring and sleep apnea by clearing or enlarging air passages, including:
- Nasal surgery to remove polyps or straighten a crooked partition between the nostrils, called a deviated septum.
- Surgery to remove enlarged tonsils or adenoids.
Lifestyle and home remedies
In many cases, self-care may be the most appropriate way for you to deal with obstructive sleep apnea. Try these tips:
- Lose weight. If you're overweight or obese, even moderate weight loss may help relieve constriction of your airway. Losing weight also can improve your health and quality of life and might reduce your daytime sleepiness.
- Exercise. Exercising, such as aerobic exercise and strength training, can help improve your condition. Aim to exercise about 150 minutes a week, and generally try to exercise most days of the week.
- Don't drink alcohol or use some anti-anxiety medicines or sleeping pills. Alcohol, some anti-anxiety medicines and some sleeping pills can worsen obstructive sleep apnea and sleepiness.
-
Sleep on your side or stomach rather than on your back. Sleeping on your back can cause your tongue and soft palate to rest against the back of your throat and block your airway.
To prevent sleeping on your back, try sewing a tennis ball in the back of your pajama top or place pillows behind you to keep you sleeping on your side.
- Keep your nasal passages open while you sleep. If you have congestion, use a saline nasal spray to help keep your nasal passages open. Talk to a member of your health care team about using nasal decongestants or antihistamines, because some medicines may be recommended for only short-term use.
Preparing for an appointment
If you suspect that you have obstructive sleep apnea, you'll likely first see your primary doctor or other health care professional. You might be referred to a sleep specialist.
Here's some information to help you get ready for your appointment.
What you can do
-
Be aware of pre-appointment requests. When you make your appointment, ask if there's anything you need to do in advance, such as keeping a sleep diary.
In a sleep diary, you record your sleep patterns such as bedtime, number of hours slept, nighttime awakenings and awake time. You also can record your daily routine, naps and how you feel during the day.
- Write down your symptoms, including any that may seem unrelated to the reason for your appointment, and when they began.
- Write down key personal information, including new or ongoing health problems, major stresses, or recent life changes.
- Bring a list of all medicines, vitamins or supplements you take, including doses. Include anything you've taken to help you sleep.
- Take your bed partner along, if possible. Your partner can provide information about how much and how well you're sleeping. If you can't bring your partner with you, ask about how well you sleep and whether you snore and then share this information at your appointment.
- Write down your questions. Preparing a list of questions can help you make the most of your time during your appointment.
For obstructive sleep apnea, some basic questions to ask include:
- What's the most likely cause of my symptoms?
- What tests do I need? Do I need to go to a sleep clinic?
- What treatments are available and which do you recommend for me?
- I have other health conditions. How can I best manage these conditions together?
Don't hesitate to ask other questions.
What to expect from your doctor
A key part of the evaluation of obstructive sleep apnea is a detailed history, meaning your health care team will ask you many questions. These may include:
- When did you first notice symptoms?
- Have your symptoms been off and on, or do you always have them?
- Do you snore? If so, does your snoring disrupt anyone else's sleep?
- Do you snore in all sleep positions or just when sleeping on your back?
- Do you ever snore, snort, gasp or choke yourself awake?
- Has anyone seen you stop breathing during sleep?
- How refreshed do you feel when you wake up? Are you tired during the day?
- Do you have a headache or dry mouth when you awaken?
- Do you doze off or have trouble staying awake while sitting quietly or driving?
- Do you nap during the day?
- Do you have family members with sleep problems?
What you can do in the meantime
- Try to sleep on your side. Most forms of obstructive sleep apnea are milder when you sleep on your side.
- Don't drink alcohol close to bedtime. Alcohol makes obstructive sleep apnea worse.
- If you're drowsy, don't drive. If you have obstructive sleep apnea, daytime sleepiness can put you at higher risk of motor vehicle accidents. To be safe, schedule rest breaks. If a close friend or family member tells you that you appear sleepier than you feel, don't drive.